CIT-38
CTier C · Extended / 3+ Step
Stress signalling pathways that impair prefrontal cortex structure and function
Arnsten, A. F. T. (2009)
Demonstrates that sympathetic overdrive and catecholamine excess (stress) actively impair Prefrontal Cortex (PFC) function. Establishes the baseline architectural premise that high-order cognitive coaching and behavioral training cannot effectively penetrate a brain locked in a biological state of survival; autonomic downregulation must occur first.
Inference:Tier C
Applicability:Extended / 3+ Step
CIT-39
BTier B · Moderate / 2-Step
Stress-related noradrenergic activity prompts large-scale neural network reconfiguration
Hermans, E. J., et al. (2011)
Demonstrates that acute systemic stress physically shifts brain connectivity away from the executive control network and toward the salience (reactive) network. Illustrates why traditional behavioral interventions frequently fail to yield long-term ROI during periods of unmanaged organizational stress — a physiological shifting mechanism equally present during clinical trauma therapy.
Inference:Tier B
Applicability:Moderate / 2-Step
CIT-40
ATier A · Strong Correlational
Heart rate variability, prefrontal neural function, and cognitive performance: the neurovisceral integration perspective
Thayer, J. F., et al. (2009)
Demonstrates that higher vagal tone (measured via HRV) is inextricably linked to superior executive function, working memory, and emotional regulation.
Inference:Tier A
Applicability:Strong Correlational
CIT-41
BTier B · Direct / 1-Step
Psychosocial stress reversibly disrupts prefrontal processing and attentional control
Liston, C., McEwen, B. S., & Casey, B. J. (2009)
Demonstrates that chronic psychosocial stress disrupts architectural connectivity in the Prefrontal Cortex. Crucially, the study proves this impairment is reversible, validating the approach of utilizing neuro-acoustic tools to restore baseline biological regulation.
Inference:Tier B
Applicability:Direct / 1-Step
CIT-42
CTier C · Moderate / 2-Step
Brain on stress: how the social environment gets under the skin
McEwen, B. S. (2012)
Indicates that chronic allostatic load induces structural remodeling in the amygdala, driving cognitive rigidity and a "defensive" posture.
Inference:Tier C
Applicability:Moderate / 2-Step
CIT-43
BTier B · Direct / 1-Step
The influence of acute stress on the regulation of conditioned fear
Raio, S. N., & Phelps, E. A. (2015)
Demonstrates that acute sympathetic arousal directly impairs the prefrontal regulation of the amygdala making cognitive behavioral interventions ineffective during high stress states.
Inference:Tier B
Applicability:Direct / 1-Step
CIT-44
BTier B · Direct / 1-Step
Heart rate variability (HRV) and posttraumatic stress disorder (PTSD): a pilot study
Tan, G., et al. (2011)
This targeted pilot study explicitly proves that implementing active autonomic downregulation (via HRV biofeedback) is an effective, feasible, and acceptable treatment for combat veterans with PTSD. Veterans with combat-related PTSD displayed significantly depressed HRV at baseline, and active physiological regulation significantly increased HRV while concurrently reducing symptoms of PTSD.
Inference:Tier C
Applicability:Direct / 1-Step
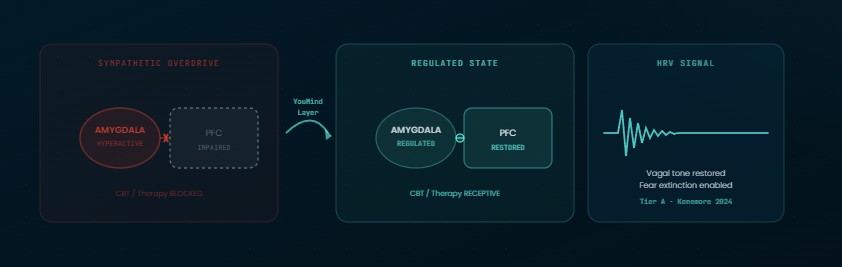
CIT-45
ATier A · Direct / 1-Step
Heart rate variability biofeedback as a treatment for military PTSD: A meta-analysis
Kenemore, J., et al. (2024)
This comprehensive meta-analysis of military service members demonstrates that establishing physiological regulation (via HRV biofeedback) produces a moderate-to-large reduction in combat PTSD symptoms. Crucially, the cumulative attrition (dropout) rate for veterans undergoing active autonomic regulation was exceptionally low (5.8%), compared to the typical 16%–36% dropout rate observed in traditional evidence-based therapies. This proves that standardizing the autonomic baseline actively mitigates Neurological Friction, drastically improving clinical compliance and retention among veterans.
Inference:Tier A (Meta-Analysis)
Applicability:Direct / 1-Step
CIT-46
BTier B · Moderate / 2-Step
Vagus nerve stimulation enhances extinction of conditioned fear and modulates plasticity in the pathway from the ventromedial prefrontal cortex to the amygdala
Peña, D. F., et al. (2014)
Demonstrates that high vagal tone and parasympathetic engagement are biological requirements for "fear extinction" — the core neurobiological mechanism required for trauma processing therapies (such as Prolonged Exposure and CBT) to succeed. Without adequate autonomic regulation, the brain cannot consolidate new "safety" memories to overwrite the trauma, rendering cognitive behavioral therapies structurally ineffective.
Inference:Tier B
Applicability:Moderate / 2-Step
CIT-47
BTier B · Direct / 1-Step
Auditory Startle Response in Trauma Survivors With Posttraumatic Stress Disorder: A Prospective Study
Shalev, A. Y., et al. (2000)
Demonstrates that the development and maintenance of PTSD are inextricably linked to progressive neuronal sensitization and exaggerated autonomic stress responses to sudden acoustic stimuli. By utilizing predictable, mathematically structured neuro-acoustic tones (isochronic rhythms), the protocol actively counteracts this acoustic sensitization, using sound to signal biological safety and bypass the hypervigilant startle reflex.
Inference:Tier B
Applicability:Direct / 1-Step